GUEST POST from Arlen Meyers
The business model canvas is one of many useful tools to design, evolve and test products and services business models. While the original model was proposed to help founders create a viable and scaleable business model, it has also helped non-profit executives, as the mission driven business model, and those looking to make a career change, using a personal business model as the Business Model You.

The construct is also useful if you are an edupreneur, trying to create and launch new educational products and services, including new courses, certificates, programs or degree offerings.
Edupreneurship rests on several foundational principles:
- Having an entrepreneurial mindset
- Intra- and entrepreneurial knowledge, skills, abilities and competencies
- Design thinking focused on creating stakeholder and beneficiary defined outcomes
- A systems engineering approach to solving wicked problems, like how to fix outcomes disparities and their social determinants
- A different business model
- More respect for and attention to edupreneurial champions
- Better teacher education and training
- An incentive and reward system for not just tweaking a failed system , but rather, making it obsolete given the basic structural changes in the US economy
- Eliminating unnecessary and burdensome bureaucracy, credentialing that does not add value and administrivia
- Paying more attention to and measuring student defined outcomes
- Better public-private integration
- K-20 integration and alignment
13. Teaching students what they need to win the 4th industrial revolution
14. Embracing cradle to career integration
15. Creating a competent diverse and equitable talent pipeline
We has seen several recent advances in edupreneurship.
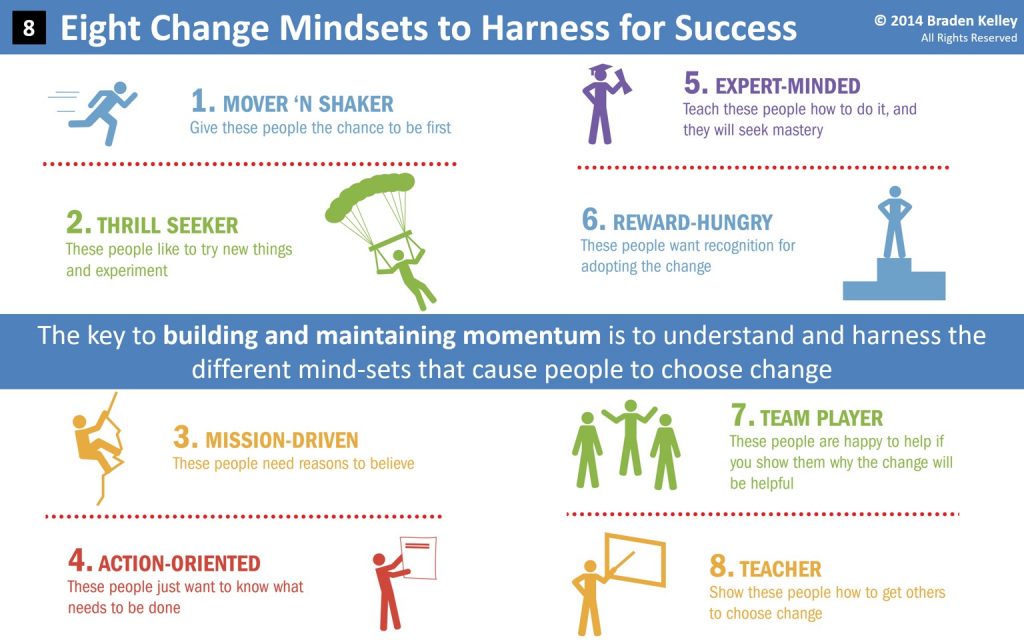
Here is the boomer’s guide to teaching millenials.
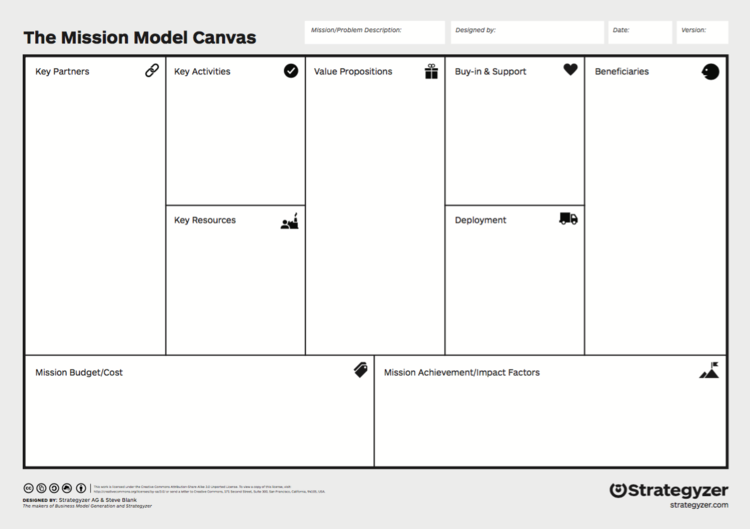
The UGME steering committee recognizes that medical education programs are faced with the ubiquitous challenge of repeated calls for innovation and that, frequently, these calls do not adequately address the associated resource demands. As medical educators, we have become highly creative in identifying strategies to do more with less, but as we know, this is not a sustainable model of stewardship. In 2016 and 2017, the UGME section collaborated with the Group on Business Affairs (GBA) to explore evolving models to support and sustain UGME programming. A result of this work is the Business Model Canvas for Medical Educators. The original Business Model Canvas was proposed by Alexander Osterwalder in 2008 and has been modified over time to fit other needs. The Table of Contents will direct you to resources, including the Business Model Canvas for Medical Educators template and two examples submitted by institutions who have successfully used the template to secure funding from within their own institution.
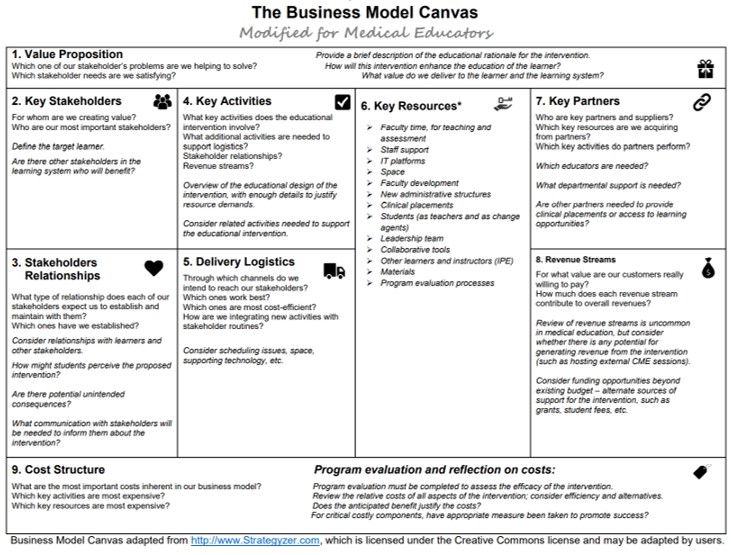
The edupreneurship business model canvas has a few modifications to the traditional startup one:
Customer segments: The primary customer are students. However, there are many other education stakeholders, including admininstrators, alumni, donors, employers and parents. In addition, for any given subject, potential students will have different backgrounds and experience in the subject, will have different jobs they want done, and, therefore, will have different applications for what they learned, be it finding a job, getting a promotion, or adding value where they presently work.
Value proposition: For each customer segment , you have a specific value proposision. You typically describe it in the course syllabus, telling users about the intended audience, the goals of the course, the learning objectives, and the curriculum. For example, the value proposition for a course I teach to xMBA/HA students is :
This course will introduce graduate level students in healthcare administration and leadership to the principles and practice of healthcare innovation and entrepreneurship defined as the pursuit of opportunity under volatile, uncertain, complex and ambiguous conditions with the goal of creating stakeholder defined value through the deployment of innovation using a valid, automatic, scaleable and time sensitive (VAST) business model.
Following completion of this course, you should be able to:
1. identify gaps in your health entrepreneurship competencies and develop a personal and professional development plan to address them
2. create an organizational culture of innovation, lead innovators and overcome the barriers to healthcare innovation dissemination and implementation
3. identify the multiple clinical and non-clinical ways to practice healthcare entrepreneurship
4. Create a plan to solve a problem inside or outside of your organization that meets the goals of the quintuple aim (Quality, cost, access, experience, waste/business operations)
5. Identify the startup life cycle and challenges at each stage
Channels: This describes how you will deliver your course. Will it be face to face, online or some hybrid model with elements of both?
Customer relationships: This describes how you will get, keep and grow the numbers of students who will take the course, e.g. promoting in the course catalog, attending a career or course proposal day, creating awareness on social media or using word or mouth dissemination from previous students.
Revenue model: This describes how your employer or you will generate revenue from the products. Traditionally, universisty based courses use a “butts in the seats” model, but COVID and new eductional technologies have radically changes the revenue generating possibilities, inluding advertising, freemium models, subscription models and others.
Key resources: This describes the human, physical, intellectual property and financial resources you will need to build, execute and scale your initiative. For example, do you want to copyright your materials, or , do you want to make them an open educational resource using a Creative Commons license?
Key activities: This what you need to do to perform and deliver on your value proposition, like what you will do using a learning management system, like create videos, run office hours, moderate asynchronous virtual discussions and design and grade exams and quizzes
Key partnerships: This describes who can help you, be they guest faculty, educational technology partners, corporate sponsors, e.g. if you are using project based learning techniques or online tools and resouce producers, e.g cases from the Harvard Business School collection.
Costs: This describes the tangible and intangible costs to produce your product. In most instances, your time, opportunity costs and effort will overshadow the monetary costs.
COVID has accelerated the pace of change in higher education, forcing them to create entrepreneurial universities. Teaching faculty how to use the education business model canvas should be part of faculty development to mimimize projecdt and product failure.
In this post , Steve Blank offers a new definition of why startups exist: a startup is an organization formed to search for a repeatable and scalable business model.
So is a new course or certificate. Use the education driven business model to make your product desireable, feasible, viable and adaptable and be sure to document your success when it comes time for your evaluation,promotion and tenure review. More likely, though, you will be including it in your failure resume, since, like the vast majority of new products, yours is likely to fail because 1) you offered a product students don’t want to buy or someone does not want to pay for, and 2) you do not have a VAST educational product business model.
Image credits: Strategyzer
![]() Sign up here to get Human-Centered Change & Innovation Weekly delivered to your inbox every week.
Sign up here to get Human-Centered Change & Innovation Weekly delivered to your inbox every week.