Have you seen the entrepreneurial mindset framework for innovation leaders?

GUEST POST from Arlen Meyers, M.D.
Most doctors, scientists, engineers, business school grads and lawyers I’ve taught don’t have an entrepreneurial mindset. There are lots of reasons why, some of which have to do with how they are chosen by their respective educational establishments. After all, you don’t get accepted to medical school because of your intense creativity. You get accepted, primarily, because of your GPA ,your performance on a standardized test, the MCAT, and how you perform in your scripted interviews.
Here are some mindset maps from Kevin Johnson:
- All risk isn’t risky. Entrepreneurs surely understand the high probability of failure, but they don’t necessarily like to gamble. Instead, they take calculated risks, stacking the deck in their favor. They must have enough confidence in themselves, supplemented by expert knowledge, solid relationships, or personal wealth, to see the risk as near zero.
- Business comes first, family second. This view isn’t a selfish one, but a recognition by serious entrepreneurs that family well-being is dependent on the success of the business, not the other way around. This is why airlines ask you to put on your oxygen mask first. Should you forego closing a million dollar deal to attend a ball game with your son?
- Following your passion is bogus. Look for a good business model first. Your passion may be for a good cause, like curing world hunger, but it may not be a good business. In any young business, you inevitably find things that are not enjoyable, but need to be done, like cold calls or firing unproductive employees. Just doing fun things is a myth.
- It’s not about being your own boss. Great entrepreneurs aren’t interested in being bosses at all. People who crave the freedom to do what they want when they want generally make terrible entrepreneurs. In order to be a successful entrepreneur, discipline is a must, and accept your new bosses as investors, partners, and customers.
- Fire your worst customers. We have all had customers who take advantage of us, to the detriment of other good customers. The best entrepreneurs are quick to make the tough decisions to bypass bad customers, with proper respect, to minimize frustration, resource drain, and reputation loss. You can’t please everyone all the time.
- Ignorance can be bliss. It’s great to be highly familiar with the industry in which you plan to compete, but many times people see too many challenges, and never start. In other cases, entrepreneurs are opening up new business areas, so no one yet knows the challenges. Serious entrepreneurs trust their ability to beat a new path to the opportunity.
- You’re in no rush to get an MBA. If you are already an entrepreneur, more education, including an MBA, will only slow you down. Consider it a waste of time. If you plan to become an entrepreneur, and already have business experience or an undergraduate business degree, skip the two-year delay and cost of the MBA.
- You are odd, and it’s OK. Entrepreneurs, especially those in technology, usually don’t start out as well-rounded, well-adjusted leaders. In fact, being odd is quite the norm. According to other studies, attention-deficit disorder (ADD) is common, as well as host of other personality disorders. It’s actually cool to be a geek in this lifestyle.
- A check in hand means nothing. Every entrepreneur remembers their naïve days when that first customer check bounced. When you receive a new purchase order, a check, a verbal agreement, or even a written agreement, don’t get too happy and excited. Save the celebration until you have cold cash in hand, or the funds are verified.
- There’s no such thing as a cold call. If you are an elite entrepreneur, you don’t go into anything cold. With the Internet and a plethora of other resources, you can warm up any call quickly, and not waste your time or theirs. Doing your homework first is one of the best ways to get an advantage over your competition.
Instead, when it comes to innovation and entrepreneurship, they have this kind of frame of reference:
- They don’t acknowledge they don’t know what they don’t know
- They don’t understand the difference between a scientific or clinical mindset and an entrepreneurial one
- They take no for an answer
- They are insecure and lack self esteem when early in their careers and therefore feel obligated to compensate with dysfunctional behaviors, often encouraged by the culture of their training programs
- They don’t take personal responsibility for their mistakes and , therefore, don’t learn from them
- They think that what got them to where they are now will get them to where they want to go
- They don’t think networking is important, so, they don’t do it
- They are not politically savvy
- They lack entrepreneurial courage
- They lack access to mentors, knowledge, education, resources, peer to peer support and career development guidance.
The entrepreneurial mindset is a state of mind interested in the pursuit of opportunity with scarce, uncontrolled resources. The goal is to create user defined value at various multiples of the existing competitive offering through the deployment of innovation.
Some describe “character” as a combination of personality, which is mostly fixed at a certain early age, and mindset, which is malleable. Character is fate.
Attitudes and motivation are what separates someone with an entrepreneurial mindset from another. The field of postive psychology has shown with overwhelming evidence that happiness creates success, not vice versa. Shawn Achor, in his book The Happiness Advantage, gives us a guided tour of the postive psychology field. noting that happiness is a positive emotion in three measurable components: pleasure, engagement and meaning. He states that happiness is the joy we feel striving after our potential. More imporantly, mindsets can change in humans from negative to positive. Consequently, happy people are primed for creativity, imagination and innovation.
Innovation starts with the right mindset and happiness makes it easier to see things clearer as well as the possibilities.
Some have described the Innovator’s DNA. Here are the amino acids that make up the genetic code.
Others note characteristics of the entrepreneurial mindset:
- Personal growth relates to the size of the challenge, not the size of the kingdom. What motivates real innovators is the more exciting challenge, not the number of people reporting to them. The ‘size of the difference’ they will make is more inspiring than the ‘size of the business.’ They relish getting out of their comfort zone, and into the unknown.
- The new direction is the challenge, not the destination. The challenge is the transformation vehicle for true innovators, and not a performance goal. They focus on legacy creation, not legacy protection. They ignore failures and are constantly looking at the progress made. They treat innovations reviews like performance reviews.
- Be an attacker of forces holding people back, not a defender. Real innovators start by questioning the world order rather than conforming to it. They begin by confronting the forces holding everyone back, rather than living with it. The forces include mindset gravity, organization gravity, industry gravity, country gravity, and cultural gravity.
- New insights come from a quest for questions, not a quest for answers. This discovery mindset searching for new questions drives real innovators away from more of the same. They fundamentally become value seekers; they look for value in every experience, in every conversation. They don’t seek prescriptions, they seek possibilities.
- Stakeholders must be connected into the new reality, not convinced. True innovators tip stakeholders into adopting and even co-owning the orbit-shifting idea. They go about tipping the heart first, assuming the mind will follow. They seek smart people, who openly express their doubts, and then collaborate to overcome them.
- Work from the challenge backward, rather than capability forward. Overcoming execution obstacles is combating dilution, not compromising, for these innovators. Their mindset is not ‘if-then’ but ‘how and how else?’ They convert problems to opportunities, and often the original idea grows far bigger than the starting promise
- Getting rid of your victim mentality.
- Having the discipline to practice the discipline
- You relish the role of leading the charge. Being a visionary or an idea person is not enough; you have to be anxious to jump in and get your hands dirty. Most success stories in business are not about envisioning the next big thing, but about making that change happen. Investors and strategic partners look for entrepreneurs who can execute.
- Able to balance right-brain and left-brain activities. Most technical entrepreneurs are left-brain logical thinkers, even perfectionists. Yet every business today needs a focus on visualization, creativity, relationships, and collaboration, which are normally in the domain of right-brainers. Successful and happy entrepreneurs have that rare whole-brain focus.
- Enjoy being outside your comfort zone. New businesses are an adventure into the unknown. You need to be mentally prepared to enjoy the roller coaster ride, rather than face it holding your breath with your teeth gritted at every turn. Only then can you enjoy the thrill of victory when you survive a major turn, and be energized for the next one.
- Proactively seek input, but make your own decisions. Great entrepreneurs seek out critical customers and industry experts, and actively listen, but are not afraid to trust their own judgment as well. Ultimately they accept the responsibility of “the buck stops here,” meaning they live by their own decisions, and never make excuses.
- Willing and able to do a little bit of everything. Technology experts tend to have a very deep level of knowledge, but not very wide. If your real interests are not very broad, then building a business will likely be frustrating and expensive. Startups have limited resources, so the founders have to enjoy trying things, and learning from their mistakes.
- Viewed by others as a successful problem solver. The best ideas for a new business are solutions to a real customer problem, rather than great ideas looking for a market. Creating a new business means tackling one difficult problem after another, until success suddenly appears. Entrepreneurs see problems as milestones to success, not barriers.
- Don’t demand or expect immediate gratification. Seth Godin once said “The average overnight success in business takes six years,” and he is an optimist. For some entrepreneurs that success is financial, and for others it is a legacy of good deeds. Because it takes so long to get there, it is important to be happy with the journey.
- Having a growth mindset. That means experimenting and letting your passion find you instead of finding your passion. Here are some tips on how to develop your growth mindset-think like employee #3 at a startup.
- Optimism Research suggests that optimists earn more money, have better relationships and even live longer. And the thing is: Optimism can be learned.
Here are the 8P’s of the Entrepreneurial Mindset:
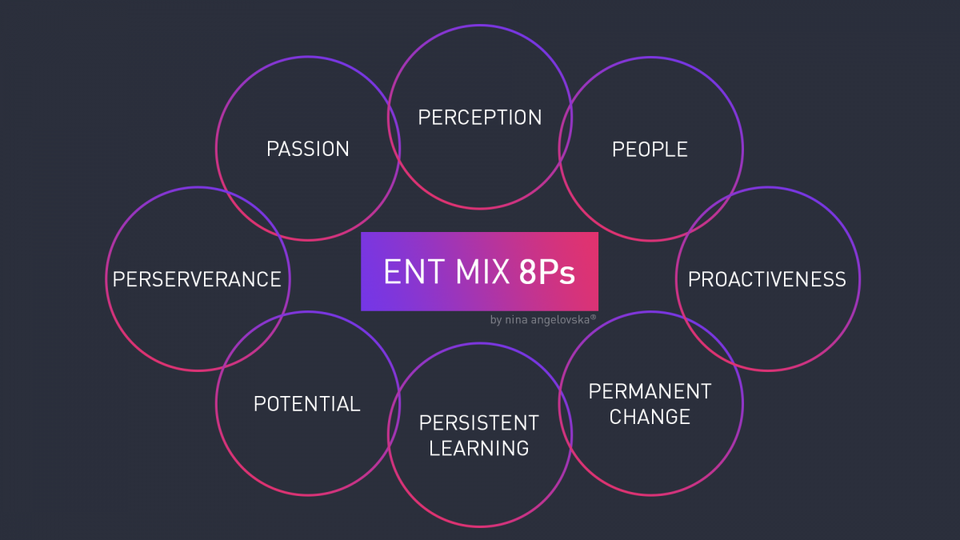
Lately, the term “grit” is popular and describes the combination of passion and perseverance. The growth mindset is driven by curiosity and self-compassion.
Here’s how the entrepreneurial mindset differs from the clinical mindset. There are also age and generational variations, e.g. how to deal with ambiguity.
Entrepreneurial mindsets derive from entrepreneurial behaviors that are part of an entrepreneurial culture. Consequently, finding entrepreneurial champions to demonstrate the mindset to others is an important tactic in changing a culture.
True innovation in sick care is rare. Ideas and inventions rarely create substantial multiples of user defined value and can be counted on one hand. Antibiotics. Anesthesia. Clean water. Transplantation.
Here are some ways to look at the world through an innovative/entrepreneurial mindset:
Wonder about inconsistencies and anomalies instead of dismissing or explaining them away.
Wonder about coincidences that seem promising.
Give freer rein to curiosity, spending more time speculating about implications of events or ideas that aren’t on the main path we are pursuing.
Be alert to unexpected connections between ideas.
Notice leverage points that might help when we get stuck – alternative ways to move forward when our usual problem-solving methods aren’t working. Instead of simply making sure projects are progressing at a satisfactory pace, supervisors can ask employees more in-depth questions: How has your understanding of the project changed? What has surprised you? Are you tempted to change the project goals? If the employee responds that nothing has to be rethought, this may indicate that the person isn’t adopting the In/Stance. Confusions and conflicts may offer opportunities for gaining insights. Employees may have misconceptions of different ideas about how things work– Investigate these inconsistencies, as they may lead to insights.
Learning is about unlearning. Like every change, it requires unfreezing , changing and refreezing.
Of course determining how many of the roughly 900,000 active docs have an entrepreneurial mindset depends on how you define it and the instrument you use to measure it. Since few, if any, have done that, including search and placement firms, there is really no valid way to know.
Here’s an article that covers the landscape and attempts to measure the entrepreneurial mindset. Basically, personalities are fixed, but skills can be learned.
Personality Scales
Independence: The desire to work with a high degree of independence (e.g., I’m uncomfortable when expected to follow others’ rules.)
Preference for Limited Structure: A preference for tasks and situations with little formal structure (e.g., I find it boring to work on clearly structured tasks.)
Nonconformity: A preference for acting in unique ways; an interest in being perceived as unique (e.g., I like to stand out from the crowd.)
Risk Acceptance: A willingness to pursue an idea or a desired goal even when the probability of succeeding is low (e.g., I’m willing to take a certain amount of risk to achieve real success.)
Action Orientation: A tendency to show initiative, make decisions quickly, and feel impatient for results (e.g., I tend to make decisions quickly.)
Passion: A tendency to experience one’s work as exciting and enjoyable rather than tedious and draining (e.g., I’m passionate about the work that I do.)
Need to Achieve: The desire to achieve at a high level (e.g., I want to be the best at what I do.)
Skill Scales
Future Focus: The ability to think beyond the immediate situation and plan for the future (e.g., I’m focused on the long term.)
Idea Generation: The ability to generate multiple and novel ideas, and to find multiple approaches for achieving goals (e.g., Sometimes the ideas just bubble out of me.)
Execution: The ability to turn ideas into actionable plans; the ability to implement ideas well (e.g., I have a reputation for being able to take an idea and make it work.)
Self-Confidence: A general belief in one’s ability to leverage skills and talents to achieve important goals (e.g., I am a self-confident person.)
Optimism: The ability to maintain a generally positive attitude about various aspects of one’s life and the world (e.g., Even when things aren’t going well, I look on the bright side.)
Persistence: The ability to bounce back quickly from disappointment, and to remain persistent in the face of setbacks (e.g., I do not give up easily.)
Interpersonal Sensitivity: A high level of sensitivity to and concern for the well-being of those with whom one works (e.g., I’m sensitive to others’ feelings.)
It would be interesting to apply this to a physician population and compare to the general one.
Teaching and learning entrepreneurship is as much about nudging students to adopt an entrepreneurial mindset as it is teaching skills, particularly if they are narrowly focused on creating a business.
But, how do you reframe a mindset? Here are some tips on how to do it.
If we are to innovate our way out the the current “health” care system mess, we need to identify those with an entrepreneurial mindset and turn them loose on the most wicked problems that beset us. Marginalizing, stifling or channeling them into a limiting culture is a terrible waste of a mindset.
Image credits: Nina Angelovska, Pixabay
 Sign up here to get Human-Centered Change & Innovation Weekly delivered to your inbox every week.
Sign up here to get Human-Centered Change & Innovation Weekly delivered to your inbox every week.